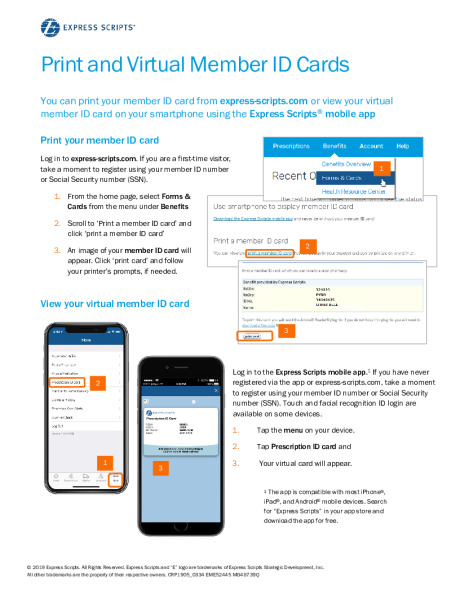
ESI RxID Card Guide English & Spanish
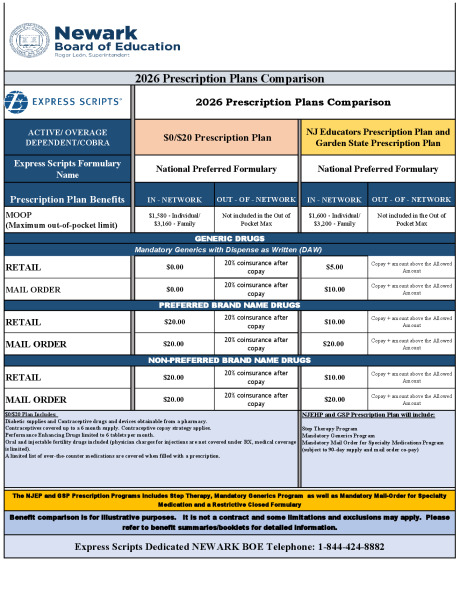
2026 Prescription Plan Comparison
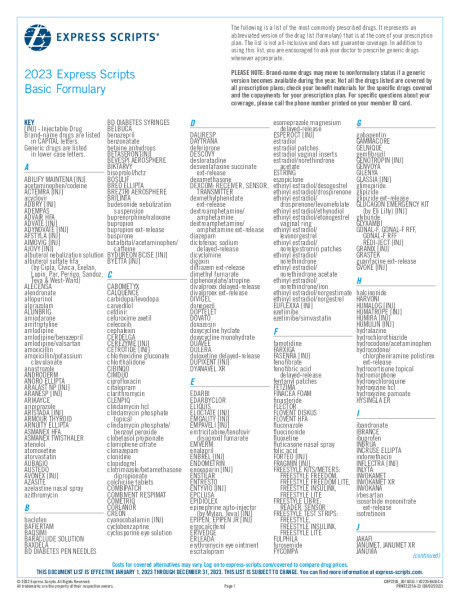
2026 ESI National Preferred Formulary Drug List
Newark Board of Education Member Packet RxBenefits
Accredo Specialty & SaveOnSP
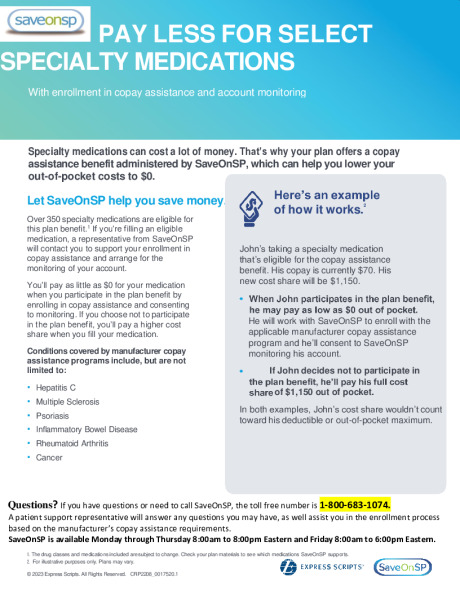
SaveOnSP Copay Assist Flyer
SaveonSP Q & A Flyer