Express Scripts Prescription Hotline number is 1-844-424-8882
NBOE does not participate with the School Employees’ Health Benefits Program administered by the State of NJ.
If you enroll onto the medical NBOE NJ Educators Plan (NJEP), or NBOE Garden State Health Plan (GSHP), prescription drug coverage is already included on the combine plan.
All medical plan participants have prescription drug coverage based on their selected plan.
A way to save money is by requesting generics and/or mail order options when available.
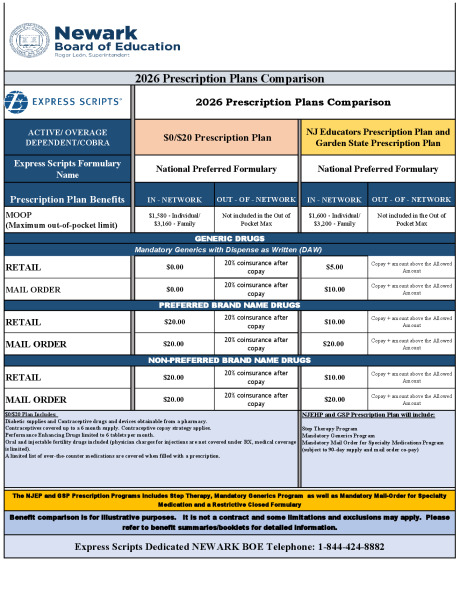
Prescription Plans Comparison
ACTIVE/ OVERAGE DEPENDENT/ COBRA
$0/$20 Prescription Plan
NJ Educators Prescription Plan and Garden State Prescription Plan
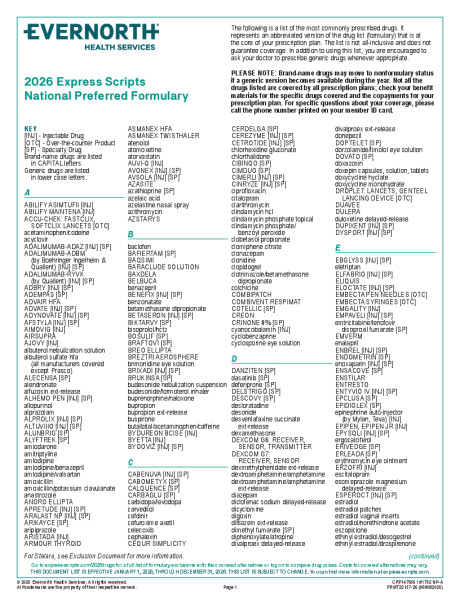
Express Scripts Formulary Name
National Formulary
National Formulary
Prescription BENEFITS
IN - NETWORK
OUT - OF - NETWORK
IN - NETWORK
OUT - OF - NETWORK
MOOP (Maximum out-of-pocket limit)
$1580 - Individual/ $3160 - Family
Not included in the Out of Pocket Max
$1,600 - Individual/ $3,200 - Family
Not included in the Out of Pocket Max
GENERIC DRUGS
Mandatory Generics with Dispense as written (DAW)
RETAIL
$0.00
20% coinsurance after copay
$5.00
Copay + amount above the Allowed Amount
MAIL ORDER
$0.00
20% coinsurance after copay
$10.00
Copay + amount above the Allowed Amount
PREFERRED BRAND NAME DRUGS
RETAIL
$20.00
20% coinsurance after copay
$10.00
Copay + amount above the Allowed Amount
MAIL ORDER
$20.00
20% coinsurance after copay
$20.00
Copay + amount above the Allowed Amount
NON-PREFERRED BRAND NAME DRUGS
RETAIL
$20.00
20% coinsurance after copay
$10.00
Copay + amount above the Allowed Amount
MAIL ORDER
$20.00
20% coinsurance after copay
$20.00
Copay + amount above the Allowed Amount
$0/$20 Plan Includes: Diabetic supplies and Contraceptive drugs and devices obtainable from a pharmacy. Contraceptives covered up to a 6 month supply. Contraceptive copay strategy applies. Performance Enhancing Drugs limited to 6 tablets per month. Oral and injectable fertility drugs included (physician charges for injections are not covered under RX, medical coverage is limited). A limited list of over-the-counter medications are covered when filled with a prescription.
NJEHP Prescription Plan will include: Step Therapy Program Mandatory Generics Program Mandatory Mail Order for Specialty Medications Program (subject to 90-day supply and mail order co-pay)
The NJEP and GSP Prescription Programs includes Step Therapy, Mandatory Generics Program as well as Mandatory Mail-Order for Specialty Medication and a Restrictive Closed Formulary (National Formulary)
Benefit comparison is for illustrative purposes. It is not a contract and some limitations and exclusions may apply. Please refer to benefit summaries/booklets for detailed information.