Which Medical Plan is Right?
Our medical carrier is Aetna. Aetna’s Medical Hotline number is 1-855-223-8791
NBOE does not participate with the School Employees’ Health Benefits Program administered by the State of NJ.
If you were hired after July 1, 2020 you can only enroll in the NBOE NJ Educators Plan (NJEP), or NBOE Garden State Health Plan (GSHP), which includes prescription coverage, Freedom of Choice Dental, and/or Vision Plan.
If you were hired before July 1, 2020, you have the option to enroll into the Legacy medical plans, and the standalone prescription coverage, and the NJEP or GSHP plan. Also, you will have access to enroll into the Freedom of Choice Dental, and/or Vision Plan.
Note: since NBOE Garden State Health Plan has a limited network, please review the information below before considering the plan.
Click here for Aetna ID Card Instructions in English & Spanish
Garden State Health Plan
Your benefits choices can have a big impact on your health care experiences and expenses, so it is important that you consider your options carefully and find the benefits that are right for you and your family. Here are a few highlights of the Garden State Health Plan with Aetna and Express Scripts:
- The GSHP uses the Aetna Whole Health℠— New Jersey network of providers.
- The GSHP offers the same level of benefit for both in and out of network services as the NJ Educators Plan (NJEP)
- The co-pays mirror the rates for the NJEP
- The GSHP plan design follows the NJEP for both Medical and Prescription Drug benefits
- The GSHP offers aВ significantly smaller network in comparison to the other plans offered in the District
- This includes only 35% of Hospitals and 60% of the Physicians in the Open Choice network
- There is no coverage for out of state providers in the GSHP, except for a true emergency.
- This includes facilities such as Memorial Sloan Kettering in NYC and CHOP in Philadelphia, which would now be considered out of network
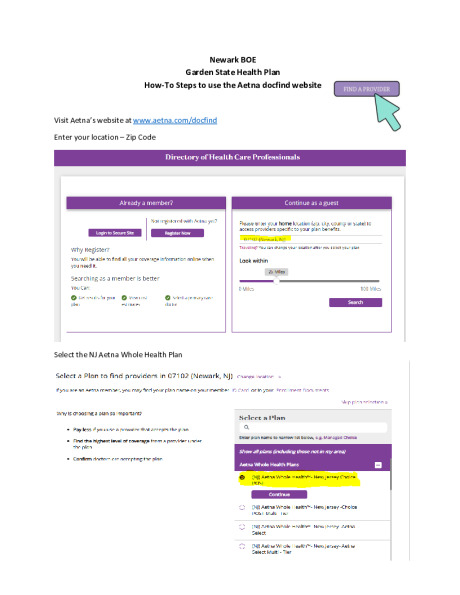
Aetna DocFind How to Steps To find a Provider under GSHP
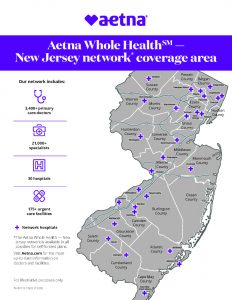
GSHP Aetna Whole Health - New Jersey network map
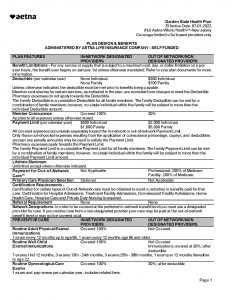
Aetna Garden State Health Plan Summary Plan
NJ Educators Plan
- The NJ Educators Plan is under the Aetna Choice POS II (Open Access) network.
- NJEP is a nationwide coverage
- NJ Educators Plan network of doctors is larger compared to the GSHP.
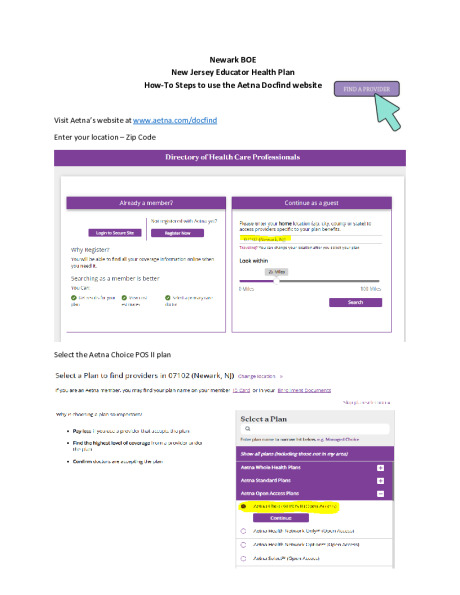
Aetna DocFind How to Steps To find a Provider under NJEHP (Choice POS II)
Medical Plan Comparison
If you were hired after July 1, 2020 you can only enroll in the NBOE NJ Educators Plan (NJEP), or NBOE Garden State Health Plan (GSHP), which includes prescription coverage, Freedom of Choice Dental, and/or Vision Plan.
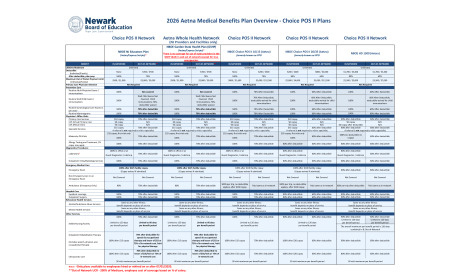
2026 Medical Benefit Grid Comparison
NJ Educators Plan (NJEP) and Garden State Health Plan (GSHP)
| NBOE NJ Educators Plan (Aetna/Express Scripts)* |
NBOE Garden State Health Plan (GSHP) (Aetna/Express Scripts)* There is no coverage for out of state providers in the GSHP (both in and out of network) except for true emergencies. |
|||||||
|---|---|---|---|---|---|---|---|---|
| BENEFIT | IN-NETWORK | OUT-OF-NETWORK** | IN-NETWORK | OUT-OF-NETWORK** | ||||
| Lifetime Maximum | Unlimited | Unlimited | ||||||
|
Deductible (Individual/Family) |
None | $350 / $700 | None | $350 / $700 | ||||
| After deductible, plan pays | 100% | 70% | 100% | 70% | ||||
|
Maximum Out of Pocket Payment Limit (Individual/Family) |
$500 / $1,000 | $2,000 / $5,000 | $500 / $1,000 | $2,000 / $5,000 | ||||
| Primary Care Physician Selection | Not Required | Not Required | ||||||
| Preventive Care | ||||||||
| Routine Adult Physician Exams / Immunizations | 100% | Not covered | 100% | Not covered | ||||
| Routine Well Child Exams / Immunizations | 100% | Well Child Exams Not Covered; Child Immunizations 70%, deductible waived |
100% | Well Child Exams Not Covered; Child Immunizations 70%, deductible waived |
||||
| Routine Gynecological Care Exams (1 per year) | 100% | 70% after deductible | 100% | 70% after deductible | ||||
| Routine Mammograms | 100% | 70% after deductible | 100% | 70% after deductible | ||||
| Physician's Office Visits | ||||||||
| Primary Care Services | $10 copay | 70% after deductible | $10 copay | 70% after deductible | ||||
| CVS Minute Clinic | $0 copay | N/A | $0 copay | N/A | ||||
| Specialist Services | $15 copay A referral is not required to visit a specialist. | 70% after deductible | $15 copay | 70% after deductible | ||||
| A referral is not required to visit a specialist. | A referral is not required to visit a specialist. | |||||||
| Maternity OB Visits | $15 copay; first visit only 100% | 70% after deductible | $15 copay; first visit only 100% | 70% after deductible | ||||
| Allergy Testing and Treatment, OV copay may apply | 100% | 70% after deductible | 100% | 70% after deductible | ||||
| Diagnostics Procedures | ||||||||
| Laboratory* | 100% in office or at Quest Diagnostics / LabCorp | 70% after deductible | 100% in office or at Quest Diagnostics / LabCorp | 70% after deductible | ||||
| Outpatient X-Ray/Radiology Services | 100% | 70% after deductible | 100% | 70% after deductible | ||||
| Emergency Medical Care | ||||||||
| Emergency Room | 100% after $125 facility copay (Copay waived if admitted) | 100% after $125 facility copay (Copay waived if admitted) | ||||||
| Non-Emergency Care in an Emergency Room | Not Covered | Not Covered | Not Covered | Not Covered | ||||
| Ambulance | 90% | 70% after deductible | 90% | 70% after deductible | ||||
| Hospital Care | ||||||||
| Inpatient coverage | 100% | 70% after deductible | 100% | 70% after deductible | ||||
| Outpatient Surgery | 100% | 70% after deductible | 100% | 70% after deductible | ||||
| Behavioral Health Services | ||||||||
| Alcohol/Substance Abuse Services | Same as any other illness; benefit depends on place of service | Same as any other illness; benefit depends on place of service | ||||||
| Mental Health Services | Same as any other illness; benefit depends on place of service | Same as any other illness; benefit depends on place of service | ||||||
| Other Services | ||||||||
| Skilled Nursing Facility | 100% | 70% after deductible | 100% | 70% after deductible | ||||
| Limited to 120 days per benefit period | Limited to 60 days per benefit period | Limited to 120 days per benefit period | Limited to 60 days per benefit period | |||||
| Outpatient Rehabilitation Therapy (includes speech, physical, and occupational therapy) | 100% after $15 copay | 70% after deductible for speech & occupational therapy and lesser of $52 or 75% of in-network cost /visit for physical therapy | 100% after $15 copay | 70% after deductible for speech & occupational therapy and lesser of $52 or 75% of in-network cost /visit for physical therapy | ||||
| Chiropractic Care | 100% after $15 copay | 70% after deductible to lesser of $35/visit or 75% of in-network cost | 100% after $15 copay | 70% after deductible to lesser of $35/visit or 75% of in-network cost | ||||
| 30 visit maximum per benefit period | 30 visit maximum per benefit period | |||||||
| Notes- *Only plans available to employees hired or rehired on or after 07/01/2020. | ||||||||
| **Out of Network UCR - 200% of Medicare, employee cost of coverage based on % of salary. | ||||||||
| Quest Diagnostics and LabCorp are the Preferred Provider for Laboratory services. | ||||||||
| “DISCLAIMER: The above is a summary of the carrier’s benefit offerings and may not reflect the plan’s finer details. Plan documents will prevail in the event of a discrepancy.” | ||||||||
Legacy Medical Plans
If you were hired before July 1, 2020, you have the option to enroll into the Legacy medical plans, and the standalone prescription coverage, and the NJEP or GSHP plan. Also, you will have access to enroll into the Freedom of Choice Dental, and/or Vision Plan.
Please see all three comparison charts below.
Choice POS II Plans (formerly known as PPO)
| Choice POS II Network | Choice POS II Network | Choice POS II Network | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NBOE Choice POS II 10/15 (Aetna) formerly known as PPO |
NBOE Choice POS II 20/35 (Aetna) formerly known as PPO |
NBOE HD 1500 (Aetna) |
||||||||||
| BENEFIT | IN-NETWORK | OUT-OF-NETWORK | IN-NETWORK | OUT-OF-NETWORK | IN-NETWORK | OUT-OF-NETWORK | ||||||
| Lifetime Maximum | Unlimited | Unlimited | Unlimited | |||||||||
| Deductible (Individual/Family) |
None | $200 / $500 | $200 / $400 | $800 / $2,000 | $1,500 / $3,000 | $1,500 / $3,000 | ||||||
| After deductible, plan pays | 100% | 70% | 80% | 60% | 80% | 60% | ||||||
| Maximum Out of Pocket Payment Limit (Individual/Family) |
$800 / $1,600 | $5,000 / $12,500 | $2,000 / $4,000 | $5,000 / $12,500 | $2,500 / $5,000 | $3,500 / $7,000 | ||||||
| Primary Care Physician Selection | Not Required | Not Required | Not Required | |||||||||
| Preventive Care | ||||||||||||
| Routine Adult Physician Exams / Immunizations | 100% | 70% After deductible | 100% | 60% After Deductible | 100% | 60% After Deductible | ||||||
| Routine Well Child Exams / Immunizations | 100% | 70% After Deductible; deductible waived for child immunizations |
100% | 60% After Deductible; deductible waived for child immunizations |
100% | 60% After Deductible; deductible waived for child immunizations |
||||||
| Routine Gynecological Care Exams (1 per year) | 100% | 70% After deductible | 100% | 60% After deductible | 100% | 60% After deductible | ||||||
| Routine Mammograms | 100% | 70% After deductible | 100% | 60% After deductible | 100% | 60% After deductible | ||||||
| Physician's Office Visits | ||||||||||||
| Primary Care Services | $10 copay | 70% after deductible | $20 copay | 60% after deductible | 80% after deductible | 60% after deductible | ||||||
| CVS Minute Clinic | $0 copay | N/A | $0 copay | N/A | $0 Copay after deductible | N/A | ||||||
| Specialist Services | $15 copay | 70% after deductible | $35 copay | 60% after deductible | 80% after deductible | 60% after deductible | ||||||
| A referral is not required to visit a specialist. | A referral is not required to visit a specialist. | A referral is not required to visit a specialist. | ||||||||||
| Maternity OB Visits | $15 copay; first visit only 100% | 70% after deductible | $35 copay; first visit only 100% |
60% after deductible | 100% (no deductible, no copay) |
60% after deductible | ||||||
| Allergy Testing and Treatment, OV copay may apply | 100% | 70% after deductible | 80% after deductible | 60% after deductible | 80% after deductible | 60% after deductible | ||||||
| Diagnostics Procedures | ||||||||||||
| Laboratory* | 100% in office or at Quest Diagnostics / LabCorp | 70% after deductible | 80% after deductible Quest Diagnostics / LabCorp |
60% after deductible | 80% after deductible Quest Diagnostics / LabCorp |
60% after deductible | ||||||
| Outpatient X-Ray/Radiology Services | 100% | 70% after deductible | 80% after deductible | 60% after deductible | 80% after deductible | 60% after deductible | ||||||
| Emergency Medical Care | ||||||||||||
| Emergency Room | 100% after $100 facility copay (Copay waived if admitted) |
80% after deductible | 60% after deductible | |||||||||
| Non-Emergency Care in an Emergency Room | Not Covered | Not Covered | Not Covered | Not Covered | Not Covered | Not Covered | ||||||
| Ambulance (emergency only) |
100% no deductible after $100 copay | 100% no deductible after $100 copay | 80% per trip, no deductible applies |
Paid same as in-network | 80% per trip after deductible | Paid same as in-network | ||||||
| Hospital Care | ||||||||||||
| Inpatient coverage | 100% | 70% after deductible | 80% after deductible | 60% after deductible | 80% after deductible | 60% after deductible | ||||||
| Outpatient Surgery | 100% | 70% after deductible | 80% after deductible | 60% after deductible | 80% after deductible | 60% after deductible | ||||||
| Behavioral Health Services | ||||||||||||
| Alcohol/Substance Abuse Services | Same as any other illness; benefit depends on place of service | Same as any other illness; benefit depends on place of service |
Same as any other illness; benefit depends on place of service |
|||||||||
| Mental Health Services | Same as any other illness; benefit depends on place of service | Same as any other illness; benefit depends on place of service |
Same as any other illness; benefit depends on place of service |
|||||||||
| Other Services | ||||||||||||
| Skilled Nursing Facility | 100% | 70% after deductible | 80% after deductible | 60% after deductible | 80% after deductible Limited to 120 days per benefit period |
60% after deductible Limited to 120 days per benefit period |
||||||
| Limited to 120 days per benefit period | Limited to 120 days per benefit period. |
The overall maximum per benefit period is 120 days combined In & Out-of-Network | ||||||||||
| Outpatient Rehabilitation Therapy (includes speech, physical, and occupational therapy) |
100% after $15 copay | 70% after deductible | 100% after $20 copay | 60% after deductible | 80% after deductible | 60% after deductible | ||||||
| Chiropractic Care | 100% after $15 copay | 70% after deductible | 100% after $20 copay | 60% after deductible | 80% after deductible | 60% after deductible | ||||||
| 30 visit maximum per benefit period | 30 visit maximum per benefit period | 30 visit maximum per benefit period | ||||||||||
| Quest Diagnostics and LabCorp are the Preferred Provider for Laboratory Services. | ||||||||||||
| DISCLAIMER: The above is a summary of the carrier’s benefit offerings and may not reflect the plan’s finer details. Plan documents will prevail in the event of a discrepancy. | ||||||||||||
Legacy Medical Plans - continued
Aetna Select Plans (Formerly HMO) - continues below
| NBOE Select 10 (Aetna) formerly known as HMO |
NBOE Select 15/25 (Aetna) formerly known as HMO |
|||||||
|---|---|---|---|---|---|---|---|---|
| IN-NETWORK | OUT-OF-NETWORK | IN-NETWORK | OUT-OF-NETWORK | |||||
| Lifetime Maximum | Unlimited | Unlimited | ||||||
|
Deductible (Individual/Family) |
None | N/A | None | N/A | ||||
| After deductible, plan pays | 100% | N/A | 100% | N/A | ||||
|
Maximum Out of Pocket Payment Limit (Individual/Family) |
$5,480 / $10,960 | N/A | $5,480 / $10,960 | N/A | ||||
| Primary Care Physician Selection | Required | Required | ||||||
| Preventive Care | ||||||||
| Routine Adult Physician Exams / Immunizations | 100% | Not Covered | 100% | Not Covered | ||||
| Routine Well Child Exams / Immunizations | 100% | Not Covered | 100% | Not Covered | ||||
| Routine Gynecological Care Exams (1 per year) | 100% | Not Covered | 100% | Not Covered | ||||
| Routine Mammograms | 100% | Not Covered | 100% | Not Covered | ||||
| Physician's Office Visits | ||||||||
| Primary Care Services | $10 copay | Not Covered | $15 copay | Not Covered | ||||
| CVS Minute Clinic | $0 copay | Not Covered | $0 copay | Not Covered | ||||
| Specialist Services | $10 copay | Not Covered | $25 copay | Not Covered | ||||
| A referral is required to visit a specialist. | A referral is required to visit a specialist. | |||||||
| Maternity OB Visits | 100% | Not Covered | 100% | Not Covered | ||||
| Allergy Testing and Treatment, OV copay may apply | 100% | Not Covered | 100% | Not Covered | ||||
| Diagnostics Procedures | ||||||||
| Laboratory* | 100% in office or at Quest Diagnostics / LabCorp |
Not Covered | 100% in office or at Quest Diagnostics / LabCorp |
Not Covered | ||||
| Outpatient X-Ray/Radiology Services | 100% | Not Covered | 100% | Not Covered | ||||
| Emergency Medical Care | ||||||||
| Emergency Room | 100% after $35 facility copay (Copay waived if admitted) |
100% after $75 facility copay (Copay waived if admitted) |
||||||
| Non-Emergency Care in an Emergency Room | Not Covered | Not Covered | Not Covered | Not Covered | ||||
| Ambulance | 100% | 100% | ||||||
| Hospital Care | ||||||||
| Inpatient coverage | 100% | Not Covered | 100% | Not Covered | ||||
| Outpatient Surgery | 100% | Not Covered | 100% | Not Covered | ||||
| Behavioral Health Services | ||||||||
| Alcohol/Substance Abuse Services | Same as any other illness; benefit depends on place of service |
Same as any other illness; benefit depends on place of service |
||||||
| Mental Health Services | Same as any other illness; benefit depends on place of service |
Same as any other illness; benefit depends on place of service |
||||||
| Other Services | ||||||||
| Skilled Nursing Facility | 100% Limited to 120 days per benefit period |
Not Covered | 100% Limited to 120 days per benefit period |
Not Covered | ||||
| Outpatient Rehabilitation Therapy (includes speech, physical, and occupational therapy) |
100% after $10 copay | Not Covered | 100% after $10 copay | Not Covered | ||||
| Chiropractic Care | 100% after office copay | Not Covered | 100% after $25 copay | Not Covered | ||||
| 20 visit maximum per benefit period | 20 visit maximum per benefit period | |||||||
| Note: Quest Diagnostics and LabCorp are the Preferred Provider for Laboratory services | ||||||||
| DISCLAIMER: The above is a summary of the carrier’s benefit offerings and may not reflect the plan’s finer details. Plan documents will prevail in the event of a discrepancy. | ||||||||
Aetna Select Plans (Formerly HMO) - continued
| NBOE Select 20/20 (Aetna) formerly known as HMO |
NBOE Select 20/35 (Aetna) formerly known as HMO |
|||||||
|---|---|---|---|---|---|---|---|---|
| BENEFIT | IN-NETWORK | OUT-OF-NETWORK | IN-NETWORK | OUT-OF-NETWORK | ||||
| Lifetime Maximum | Unlimited | Unlimited | ||||||
|
Deductible (Individual/Family) |
None | N/A | $200 / $400 | N/A | ||||
| After deductible, plan pays | 100% | N/A | 80% | N/A | ||||
|
Maximum Out of Pocket Payment Limit (Individual/Family) |
$5,480 / $10,960 | N/A | $2,000 / $4,000 | N/A | ||||
| Primary Care Physician Selection | Required | Required | ||||||
| Preventive Care | ||||||||
| Routine Adult Physician Exams / Immunizations | 100% | Not Covered | 100% | Not Covered | ||||
| Routine Well Child Exams / Immunizations | 100% | Not Covered | 100% | Not Covered | ||||
| Routine Gynecological Care Exams (1 per year) | 100% | Not Covered | 100% | Not Covered | ||||
| Routine Mammograms | 100% | Not Covered | 100% | Not Covered | ||||
| Physician's Office Visits | ||||||||
| Primary Care Services | $20 copay | Not Covered | $20 copay | Not Covered | ||||
| CVS Minute Clinic | $0 copay | Not Covered | $0 copay | Not Covered | ||||
| Specialist Services | $20 copay | Not Covered | $35 copay | Not Covered | ||||
| A referral is required to visit a specialist. | A referral is required to visit a specialist. | |||||||
| Maternity OB Visits | 100% | Not Covered | 100% | Not Covered | ||||
| Allergy Testing and Treatment | 100% | Not Covered | 100% | Not Covered | ||||
| Diagnostics Procedures | ||||||||
| Laboratory* | 100% in office or at Quest Diagnostics / LabCorp |
Not Covered | 100% in office or at Quest Diagnostics / LabCorp |
Not Covered | ||||
| Outpatient X-Ray/Radiology Services | 100% | Not Covered | 100% | Not Covered | ||||
| Emergency Medical Care | ||||||||
| Emergency Room | 100% after $100 facility copay (Copay waived if admitted) |
100% after $100 facility copay (Copay waived if admitted) |
||||||
| Non-Emergency Care in an Emergency Room | Not Covered | Not Covered | Not Covered | Not Covered | ||||
| Ambulance | 100% | 100% after $100 copay | ||||||
| Hospital Care | ||||||||
| Inpatient coverage | 100% | Not Covered | 100% | Not Covered | ||||
| Outpatient Surgery | 100% | Not Covered | 100% | Not Covered | ||||
| Behavioral Health Services | ||||||||
| Alcohol/Substance Abuse Services | Same as any other illness; benefit depends on place of service |
Same as any other illness; benefit depends on place of service |
||||||
| Mental Health Services | Same as any other illness; benefit depends on place of service |
Same as any other illness; benefit depends on place of service |
||||||
| Other Services | ||||||||
| Skilled Nursing Facility | 100% Limited to 120 days per benefit period |
Not Covered | 80% after deductible Limited to 120 days per benefit period |
Not Covered | ||||
| Outpatient Rehabilitation Therapy | 100% after $20 copay | Not Covered | 100% after $20 copay | Not Covered | ||||
| (includes speech, physical, and occupational therapy) | 60 visit maximum per benefit period combined In and Out-of-Network |
100% after $20 copay | Not Covered | |||||
| Chiropractic Care | 100% after office $20 copay | Not Covered | 100% after $25 copay | Not Covered | ||||
| 20 visit maximum per benefit period | 20 visit maximum per benefit period | |||||||
| Note: Quest Diagnostics and LabCorp are the Preferred Provider for Laboratory services | ||||||||
| DISCLAIMER: The above is a summary of the carrier’s benefit offerings and may not reflect the plan’s finer details. Plan documents will prevail in the event of a discrepancy. | ||||||||
Video: Preventative Care